An Unanswered Need …
PANSURAS originated in an insight into an evident need for change in the current systems of preoperative surgical risk assessment — a solution eliminating many of the perceptions, deficiencies and lacunae in current preoperative assessment practice.
The need … Perceptions, deficiencies and lacunae
Most physicians at this moment, among which surgeons and anesthesiologists, unknowingly fail to realize the truly vast lack of real knowledge about which risk factors are relevant for each particular type of surgery in their locality. This sounds bombastic and negative, but is generally true. So, what are these perceptions, deficiencies and lacunae needing answers and correction?
- Nearly all current perioperative assessment is based upon a simple premise expressed as, “The more comorbidity, the higher the risk.” But is this true for all operations? For example, compare the relevance of multiple comorbidities for a patient requiring an open abdominal aorta reconstruction, versus the same patient requiring a dental filling.
- Uncertainty as to the relevance of risk factors for specific operations. Examples of risk factors whose individual relevance is uncertain are: heart murmurs, basal crackles, gait, orthopnea, etc. Once again, the same questions arise as to the real relevance of each comorbidity to a specific operative procedure.
- Inappropriate assessment of risk factors. Are risk factors for postoperative outcomes after a specific operation the same as those for a different operation?
- Cross-cultural inappropriateness. Physicians generalize from risk-factors derived in one part of the world to patients in other parts of the world. But it is very questionable whether risk factors for perioperative outcomes after a specific operation are the same in all parts of the world?
- Furthermore, if there are some identical risk factors for a postoperative outcome after a specific operation: is the weighting of these risk factors identical in different parts of the world?
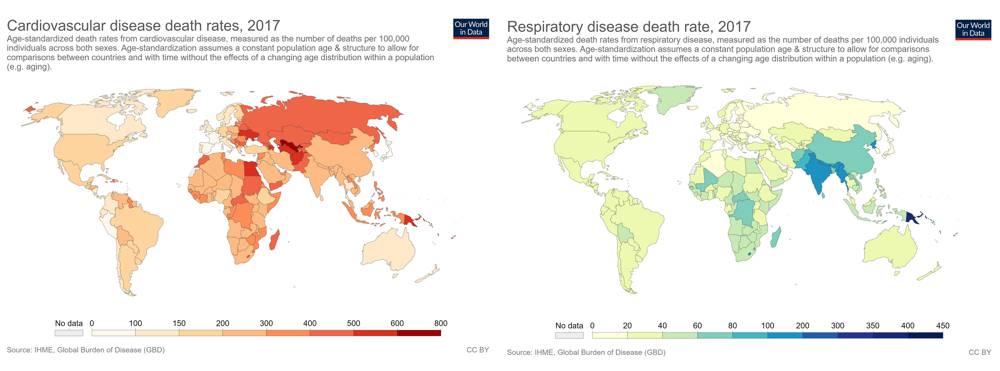
The “Global Burden of Disease” studies (See article here) reveal marked differences in comorbidity profiles between different parts of the the world. These will express themselves as differences in risk factors and weightings of the same risk factors for any given surgical procedure. (Click image to enlarge)
|
- Inappropriate generalization of modern risk prediction algorithms. A good example is the application of the modern American College of Surgeons risk calculator based upon data from 400+ top-clinical hospitals in the USA (Bilimoria 2013, Irani 2014). This risk calculator is even inaccurate when applied to hospitals other than the 400+ top clinical hospitals in the USA (Adegboyega 2017). Furthermore, the serious question arises whether the same predictive system is relevant in hospitals in other parts of the world, such as: Alice Springs in Australia, or Ahmedabad in India, or Mombasa in Kenya.
- Inappropriate use of old predictive algorithms. An example is the continued use of the POSSUM score (Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity). This score was first published during 1991 (Copeland 1991), and revised somewhat during 1998 (Prytherch 1998). This predictive and quality system was derived in both cases from clinically admitted English public health system patients who underwent general surgical procedures. Surgical practice and perioperative management have undergone major changes during the last 20 years, so it is doubtful whether this algorithm is even still relevant for English public health system patients, without even considering its relevance in other countries.
- Modern preoperative assessment is seldom designed for any specific locality, is qualitative and not quantitative, as well as varying somehwat with the physician performing the assessment. This renders understanding of these perceptions, deficiencies and lacunae very relevant indeed. Nonetheless, current qualitative systems fail to perform as efficiently, or to drive improvements in perioperative quality of care as would a quantitatively based machine-learning system.
PANSURAS is a secure (NEN 7510 / ISO 27001 / GDPR compliant) cloud-based solution to all the above deficiencies and lacunae, faciltitating ERAS (Enhanced Recovery After Surgery) by making rapid improvements in perioperative care possible.
References:
- Adegboyega T.O., et al, (2017), Applying the National Surgical Quality Improvement Program risk calculator to patients undergoing colorectal surgery: theory vs reality. The American Journal of Surgery, 213: 30-35.
- Bilimoria K.Y, et al, (2013), Development and Evaluation of the Universal ACS NSQIP Surgical Risk Calculator: A Decision Aid and Informed Consent Tool for Patients and Surgeons. Journal of the American College of Surgeons. 217: 833-842.
- Copeland G.P., et al, (1991), POSSUM: a scoring system for surgical audit. British Journal of Surgery, 78: 356-360.
- Irani J.L., (2014), Participation in Quality Measurement Nationwide. Clinics in Colon and Rectal Surgery, 27: 14-18.
- Prytherch D.R., et al, (1998), POSSUM and Portsmouth POSSUM for predicting mortality. British Journal of Surgery, 85: 1217-1220.